I’ve been asked many times about the difference between electrons and superficial X-rays when we use radiotherapy treatment for Dupuytren’s and Ledderhose disease. I have therefore written this blog post to write about how they both work, with particular notes on the similarities and differences between them.
Fundamentally, how does radiotherapy affect tissues?
Tissue is made up of atoms, each of which consists of a small positively-charged nucleus, surrounded by a swarm of negatively-charged electrons. Radiation passing through tissue interacts with these electrons, and if the radiation has enough energy, it is capable of knocking electrons away from around their atoms.
Losing a negatively-charged electron turns a neutral atom into a positively-charged ion, a process known as ionisation. If enough energy is transferred to the departing electron, it may in turn knock electrons out of surrounding atoms, causing a “cascade” of ionisation.
Ionisation of water molecules in the cell can create ions called free radicals, which are highly reactive. Their reaction with atoms within a DNA molecule (which carries the genetic material for a cell), which can damage the DNA enough to kill the cell.
Radiation capable of causing this effect is known as ionising radiation, and both X-rays and high-energy electron beams fall into this category.
The differences & similarities between electrons & X-rays
Both affect tissues in similar ways, and actually have exactly the same effect dose-for-dose on the tissues (whether that is disease or normal tissues). The differences are:
1. They are delivered by different machines
Electrons are delivered by very complex and expensive machines. The treatment is delivered from afar, which requires the hand or foot to remain very still (i.e. to be immobilised) when the radiotherapy is given. The “shielding” (material which stops the radiotherapy being given to the areas where it is not required) is within the head of the machine, so that it is not visible to the patient.
Superficial radiotherapy is delivered by a much simpler machine, and the head of the machine is placed near to the body. In fact, the end of the machine generally touches the hand or foot, and the shielding consists of lead cut-outs (shapes or strips) that are placed on the patient’s hand or foot so that the radiation does not affect the areas that it is not required to treat.
2. The physical characteristics of the radiation are different
When marking a patient up for electron treatment, the doctor will add a larger margin around the disease to ensure that the full dose is delivered to the disease. So, for instance, the doctor may mark the disease and add 2.0 cm with electrons, as opposed to1.5 cm around it with X-rays.
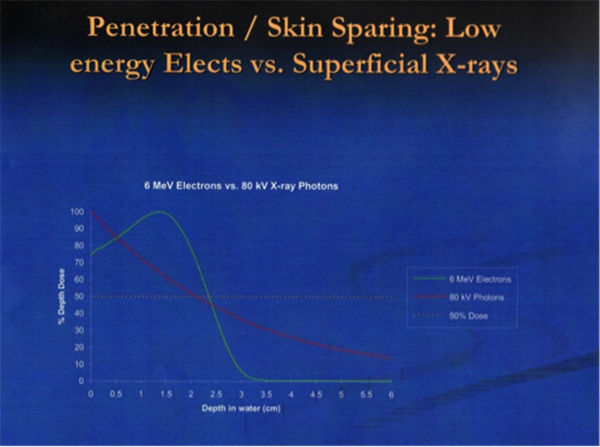
The dose at various depths is different with the two types of treatment, as seen in the “depth-dose curves” below. Firstly, with X-rays, the full dose is delivered at the surface, with a slow drop-off of dose below the surface as it is absorbed by the tissues. In contrast, with electrons, the full dose is not delivered at the surface, so wax (“bolus”) is put on the skin to artificially raise the surface dose. Also, the drop-off of the electron dose is sharper than that of X-rays, although for hands and feet these differences are unlikely to be clinically relevant.